Ranging from mild to painful disorders, more than a third of all Australians over 45 years of age may be affected by diverticulosis or diverticulitis.
Diverticulosis vs diverticulitis: learn the differences
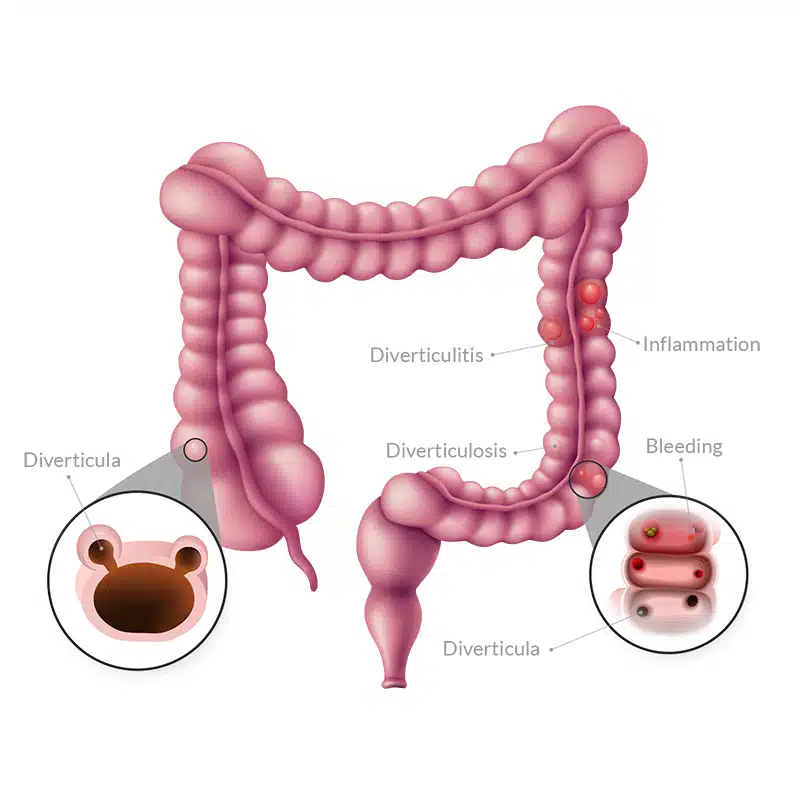
Diverticulosis occurs when random parts of the muscles lining the large intestine or colon form small pouches, called diverticula.
Diverticulitis occurs when the intestinal diverticula become infected and inflamed.
Together, diverticulosis and diverticulitis are commonly known as diverticular disease, and they are common conditions among certain age groups.
How common is diverticulosis and diverticulitis?
- As you age, your chances of developing diverticulosis or diverticulitis increase: more than 65% of older adults (over 85 years of age) develop some form of diverticular disease1.
- Diverticulosis and diverticulitis represent an important health burden, costing healthcare systems billions and causing as many as 23,000 deaths per year in Europe2-3.
What are some typical symptoms of diverticulosis and diverticulitis?
- For most people, diverticulosis is a condition with no evident symptoms.
- However, when the number of intestinal pouches (diverticula) increases, the condition can affect the normal functioning of the intestine.
- Symptoms associated with diverticulosis include:
- abdominal pain and bloating,
- constipation or diarrhoea,
- flatulence, and
- bloody stools.
- In some people, diverticulosis can develop into diverticulitis, where the intestinal diverticula become infected and inflamed.
- Diverticulitis can cause symptoms like:
- A sharp, localised pain in the abdominal area.
- Fever
- Nausea, and vomiting.
Important: Diverticulitis is considered a medical emergency and requires immediate hospitalisation.
Are you likely to get diverticulosis or diverticulitis?
- Are male – a study found that, on average, males develop complications related to diverticulosis or diverticulitis five years earlier than women4.
- Are overweight or obese – a study found that obese people were 1.4 more likely to develop diverticulosis5.
- Follow a low-fibre diet, high in fat and poor-quality red meat.
- Don’t exercise.
- Take nonsteroidal anti-inflammatory drugs (NSAIDs), like aspirin or ibuprofen.
What causes diverticulosis and diverticulitis?
Underlying factors of diverticulosis and diverticulitis
While there is no clear understanding of the causes behind diverticulosis and diverticulitis, genetics has been established as an important underlying factor6-7. Other important underlying factors that have been identified include:
Chronic inflammation occurring in and around diverticula has been strongly associated with diverticular diseases like Symptomatic Uncomplicated Diverticular Disease and acute diverticulitis8.
Abnormal colon motility is another problem tightly associated with diverticular disease. People with diverticular disease have been shown to have physiological problems like “spastic colon”, where there is an excess of contractions9. Also, anatomical issues, like reduced density of certain cells has been identified in patients with diverticular disease10.
- For example, the SCFA butyrate, commonly produced by certain strains of gut bacteria has been shown to decrease the risk of recurrent diverticulitis13.
- Studies have shown that people with a history of acute diverticulitis have a gut microbiota composition that is different from that of people with diverticulosis or with other intestinal conditions (Table 1).
[table id=2/]
aIncrease in bacterial levels occur on the underlined condition.
What factors increase the risk of diverticulosis and diverticulitis?
Below are further details about the key factors associated with the development of diverticulosis and diverticulitis:
- Fibre – a high fibre diet has been associated with decreased risk of hospitalisation by diverticular diseases20. However, more research in this area is needed to fully understand the role of fibre in this condition.
- Vitamin D – this is an important micronutrient involved in the maintenance of homeostasis in the colon through the regulation of inflammation. Supplementation of Vitamin D has been shown to a reduction in the risk of developing diverticulitis21.
- Red Meat – high consumption of red meat is a high-risk factor in colon cancer obesity. Now, red meat has also been linked to higher risk of diverticular disease by some studies22-23.
It is important to reduce your stress levels, as studies show that stress activates inflammatory pathways in the intestine24.
It is important to reduce your stress levels, as studies show that stress activates inflammatory pathways in the intestine24.
A recent review that evaluated multiple research reports concluded that even small increased in your ideal Body Mass Index (BMI) may increase your risk of developing diverticular disease. Likewise, this review found that regular exercise reduces this risk27-28.
Use of over-the-counter and prescription drugs, like opiate analgesics, corticosteroids and nonsteroidal anti-inflammatory drugs (NSAIDs) has been shown to increase the severity of diverticular diseases. Among these NSAIDs, such as aspirin and ibuprofen have shown strong evidence for their role worsening diverticular diseases, leading to conditions like diverticular perforation, diverticular bleeding or diverticulitis29-31.
How are they diagnosed?
Diverticulitis – If you are suffering from diverticulitis, you will experience symptoms typical of this condition and it is important that you visit a health care provider immediately. Typical assessment of diverticulitis include:
- Evaluation of medical history
- Laboratory testing, including blood, stools
- Visual inspection of the colon, which may include different tests, including CT scans, X-ray scan, colonoscopy, and sigmoidoscopy.
- Initially, your doctor may also perform a manual inspection of the rectum area.
- If you are experiencing rectal bleeding, you may receive an angiography, where a dye is injected to the arteries associated with the colon, to identify where the bleeding is occurring.
Treatment of diverticulosis and diverticulitis
Treatment of diverticulosis and diverticulitis depends on the severity of the condition. For example, most patients who are only experiencing the development of diverticula will not progress to a more serious condition. Hence, these patients do not receive any pharmacological treatment. Below are some examples of standard treatments for different diverticular diseases:
Patients with this condition can be treated with a high-fibre diet32-33, antibiotics34, anti-inflammatory drugs such as mesalazine or balsalazide35 and probiotics36.
Treatment for this condition depends on the severity of the disease, as patients can exhibit uncomplicated diverticulitis, diverticulitis complicated with abscess, perforation or peritonitis. The standard treatment involves anti-microbial treatment, but some patients may require surgery12, 37.
An extensive review of standard treatments of diverticular diseases can be found here.
Prevention of diverticulosis and diverticulitis
Detecting and treating modifiable risk factors associated with diverticulosis and diverticulitis will result in significant benefits to your health and will help prevent the development of diverticulosis and diverticulitis. Some of the key factors involved with diverticulosis and diverticulitis include:
For example, obesity, physical inactivity, and a Western diet are all factors associated with diverticulosis and diverticulitis and they are also risk factors for conditions like cardiovascular disease, diabetes or IBD – all diseases with established links to chronic inflammation37-38.
All of these factors, obesity, physical inactivity, and a Western die, are modifiable, meaning that a patient can make changes to their lifestyle to improve them39-40. Changing to a healthier diet (rich in fibre and low in fats and sugar) and increasing levels of exercise will result in multiple benefits, reducing systemic and chronic inflammation and improving you’re the overall function of your body41.
- A recent study showed that following a diet low in carbohydrates and high in healthy fats (keto diets) can influence the composition of the gut microbiota and reduce levels of inflammation. Read about this study in our Journal article: “Keto Diet, Gut Microbiota and Inflammation: new link identified”.
- Increasing consumption of certain types of fibre, like resistant starch can promote the formation of a healthy gut microbiota. Another benefit of consuming optimal levels of resistant starch is that it promotes the production of short chain fatty acids chemicals produced by gut bacteria. These chemicals are the main source of energy for colonocytes, cells that make up the colon wall, promoting their growth, differentiation and optimal function. Read our Journal article: “Short Chain Fatty Acids: the chemical language of the gut microbiota.”
- Small intestinal bacterial overgrowth (SIBO) commonly affects patients with diverticulosis and diverticulitis. Treatment of SIBO has been shown to result in improved outcomes for patients with diverticulosis and diverticulitis. Learn more about SIBO with our Journal article: “Understanding SIBO (Small Intestinal Bacterial Overgrowth): a hard to treat condition”.
- Intake of prebiotics and probiotics can help supplement a health diet and improve the growth and function of intestinal bacteria associated with positive health outcomes. Learn more about prebiotics and probiotics with our Journal Article: “Prebiotics vs probiotics, which one is right for your gut?”.
- A recent study showed that following a diet low in carbohydrates and high in healthy fats (keto diets) can influence the composition of the gut microbiota and reduce levels of inflammation. Read about this study in our Journal article: “Keto Diet, Gut Microbiota and Inflammation: new link identified”.
- Increasing consumption of certain types of fibre, like resistant starch can promote the formation of a healthy gut microbiota. Another benefit of consuming optimal levels of resistant starch is that it promotes the production of short chain fatty acids chemicals produced by gut bacteria. These chemicals are the main source of energy for colonocytes, cells that make up the colon wall, promoting their growth, differentiation and optimal function. Read our Journal article: “Short Chain Fatty Acids: the chemical language of the gut microbiota.”
- Small intestinal bacterial overgrowth (SIBO) commonly affects patients with diverticulosis and diverticulitis. Treatment of SIBO has been shown to result in improved outcomes for patients with diverticulosis and diverticulitis. Learn more about SIBO with our Journal article: “Understanding SIBO (Small Intestinal Bacterial Overgrowth): a hard to treat condition”.
- Intake of prebiotics and probiotics can help supplement a health diet and improve the growth and function of intestinal bacteria associated with positive health outcomes. Learn more about prebiotics and probiotics with our Journal Article: “Prebiotics vs probiotics, which one is right for your gut?”.
- Reducing levels of stress, which contributes to reducing levels of chronic inflammation.
- Following an optimal diet, designed by a dietician. This may include increasing consumption of nuts, fibre, and reducing intake of poor-quality red meats and fats as well as avoiding all refined foods.
- Improve your lifestyle – this includes increasing your levels of physical activity, reducing your BMI, reducing your waist-to-hip ratio, not smoking.
- Avoid certain medications – non- aspirin NSAIDs, aspirin, all NSAIDs, corticosteroids, and opiate analgesics should be avoided whenever possible.
- Taking prebiotics, minerals supplements and probiotics, consulting with your AUSCFM practitioner for a personalised plan.
- Evaluating the health of your gut microbiota, consult with our expert team at AUSCFM.
a Functional Medicine approach
Our approach is evidence-based and is backed by comprehensive state-of-the-art testing of all relevant factors that influence diverticulosis and diverticulitis. Our therapies are evidence-based, and rely on a combination of standard medical approaches and modern functional medicine, which combines medications, with natural supplements and lifestyle changes.
We consider the symptoms and problems you report but we also investigate potential problems you may not be aware of, hence building a complete picture of your pathology. Become a patient today!
References
- Boynton W, Floch M. New strategies for the management of diverticular disease: insights for the clinician. Therapeutic advances in gastroenterology. 2013 May;6(3):205-13. Read it!
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ, Gangarosa LM, Thiny MT, Stizenberg K, Morgan DR, Ringel Y. Burden of gastrointestinal disease in the United States: 2012 update. Gastroenterology. 2012 Nov 1;143(5):1179-87. Read it!
- Delvaux M. Diverticular disease of the colon in Europe: epidemiology, impact on citizen health and prevention. Alimentary pharmacology & therapeutics. 2003 Nov;18:71-4. Read it!
- McConnell EJ, Tessier DJ, Wolff BG. Population-based incidence of complicated diverticular disease of the sigmoid colon based on gender and age. Dis Colon Rectum. 2003 Aug;46(8):1110-4. doi: 10.1007/s10350-004-7288-4. PMID: 12907908. Read it!
- Wijarnpreecha, Karn; Ahuja, Wasin; Chesdachai, Supavit; Thongprayoon, Charat; Jaruvongvanich, Veeravich; Cheungpasitporn, Wisit; Ungprasert, Patompong. Obesity and the Risk of Colonic Diverticulosis: A Meta-analysis, Diseases of the Colon & Rectum: April 2018 – Volume 61 – Issue 4 – p 476-48. Read it!
- Reichert MC, Lammert F. The genetic epidemiology of diverticulosis and diverticular disease: Emerging evidence. United European gastroenterology journal. 2015 Oct;3(5):409-18. Read it!
- Maguire LH, Handelman SK, Du X, Chen Y, Pers TH, Speliotes EK. Genome-wide association analyses identify 39 new susceptibility loci for diverticular disease. Nature genetics. 2018 Oct;50(10):1359-65. Read it!
- Tursi A, Elisei W. Role of inflammation in the pathogenesis of diverticular disease. Mediators of inflammation. 2019 Mar 14;2019. Read it!
- Bassotti G, Sietchiping-Nzepa F, de Roberto G, Chistolini F, Morelli A. Colonic regular contractile frequency patterns in irritable bowel syndrome: the ‘spastic colon’revisited. European journal of gastroenterology & hepatology. 2004 Jun 1;16(6):613-7. Read it!
- Bassotti G, Battaglia E, Bellone G, Dughera L, Fisogni S, Zambelli C, Morelli A, Mioli P, Emanuelli G, Villanacci V. Interstitial cells of Cajal, enteric nerves, and glial cells in colonic diverticular disease. Journal of clinical pathology. 2005 Sep 1;58(9):973-7. Read it!
- Koh A, De Vadder F, Kovatcheva-Datchary P, Bäckhed F. From dietary fiber to host physiology: short-chain fatty acids as key bacterial metabolites. Cell. 2016 Jun 2;165(6):1332-45. Read it!
- Krokowicz L, Stojcev Z, Kaczmarek BF, Kociemba W, Kaczmarek E, Walkowiak J, Krokowicz P, Drews M, Banasiewicz T. Microencapsulated sodium butyrate administered to patients with diverticulosis decreases incidence of diverticulitis—a prospective randomized study. International Journal of Colorectal Disease. 2014 Mar 1;29(3):387-93. Read it!
- Hullar MA, Sandstrom R, Lampe JW, Strate LL. The fecal microbiome differentiates patients with a history of diverticulitis vs those with uncomplicated diverticulosis. Gastroenterology. 2017 Apr 1;152(5):S624. Read it!
- Daniels L, Budding AE, de Korte N, Eck A, Bogaards JA, Stockmann HB, Consten EC, Savelkoul PH, Boermeester MA. Fecal microbiome analysis as a diagnostic test for diverticulitis. European journal of clinical microbiology & infectious diseases. 2014 Nov 1;33(11):1927-36. Read it!
- Barbara G, Scaioli E, Barbaro MR, Biagi E, Laghi L, Cremon C, Marasco G, Colecchia A, Picone G, Salfi N, Capozzi F. Gut microbiota, metabolome and immune signatures in patients with uncomplicated diverticular disease. Gut. 2017 Jul 1;66(7):1252-61. Read it!
- Kvasnovsky CL, Leong LE, Choo JM, Abell GC, Papagrigoriadis S, Bruce KD, Rogers GB. Clinical and symptom scores are significantly correlated with fecal microbiota features in patients with symptomatic uncomplicated diverticular disease: a pilot study. European journal of gastroenterology & hepatology. 2018 Jan 1;30(1):107-12. Read it!
- Tursi A, Mastromarino P, Capobianco D, Elisei W, Miccheli A, Capuani G, Tomassini A, Campagna G, Picchio M, Giorgetti G, Fabiocchi F. Assessment of fecal microbiota and fecal metabolome in symptomatic uncomplicated diverticular disease of the colon. Journal of clinical gastroenterology. 2016 Oct 1;50:S9-12. Read it!
- Crowe FL, Appleby PN, Allen NE, Key TJ. Diet and risk of diverticular disease in Oxford cohort of European Prospective Investigation into Cancer and Nutrition (EPIC): prospective study of British vegetarians and non-vegetarians. Bmj. 2011 Jul 19;343:d4131. Read it!
- Tursi A, Scarpignato C, Strate LL, Lanas A, Kruis W, Lahat A, Danese S. Colonic diverticular disease. Nature Reviews Disease Primers. 2020 Mar 26;6(1):1-23. Read it!
- Carabotti M, Annibale B, Severi C, Lahner E. Role of fiber in symptomatic uncomplicated diverticular disease: a systematic review. Nutrients. 2017 Feb;9(2):161. Read it!
- Maguire LH, Song M, Strate LE, Giovannucci EL, Chan AT. Higher serum levels of vitamin D are associated with a reduced risk of diverticulitis. Clinical Gastroenterology and Hepatology. 2013 Dec 1;11(12):1631-5. Read it!
- Cao Y, Strate LL, Keeley BR, Tam I, Wu K, Giovannucci EL, Chan AT. Meat intake and risk of diverticulitis among men. Gut. 2018 Mar 1;67(3):466-72. Read it!
- Strate LL, Keeley BR, Cao Y, Wu K, Giovannucci EL, Chan AT. Western dietary pattern increases, and prudent dietary pattern decreases, risk of incident diverticulitis in a prospective cohort study. Gastroenterology. 2017 Apr 1;152(5):1023-30. Read it!
- Collins SM. IV. Modulation of intestinal inflammation by stress: basic mechanisms and clinical relevance. American Journal of Physiology-Gastrointestinal and Liver Physiology. 2001 Mar 1;280(3):G315-8. Read it!
- Turunen P, Wikström H, Carpelan-Holmström M, Kairaluoma P, Kruuna O, Scheinin T. Smoking increases the incidence of complicated diverticular disease of the sigmoid colon. Scandinavian Journal of Surgery. 2010 Mar;99(1):14-7. Read it!
- Aune D, Sen A, Leitzmann MF, Tonstad S, Norat T, Vatten LJ. Tobacco smoking and the risk of diverticular disease–a systematic review and meta‐analysis of prospective studies. Colorectal Disease. 2017 Jul;19(7):621-33. Read it!
- Aune D, Sen A, Leitzmann MF, Norat T, Tonstad S, Vatten LJ. Body mass index and physical activity and the risk of diverticular disease: a systematic review and meta-analysis of prospective studies. European journal of nutrition. 2017 Dec 1;56(8):2423-38. Read it!
- Jansen A, Harenberg S, Grenda U, Elsing C. Risk factors for colonic diverticular bleeding: a Westernized community based hospital study. World journal of gastroenterology: WJG. 2009 Jan 28;15(4):457. Read it!
- Hjern F, Mahmood MW, Abraham‐Nordling M, Wolk A, Håkansson N. Cohort study of corticosteroid use and risk of hospital admission for diverticular disease. British Journal of Surgery. 2015 Jan;102(1):119-24. Read it!
- Kvasnovsky CL, Papagrigoriadis S, Bjarnason I. Increased diverticular complications with nonsteriodal anti‐inflammatory drugs and other medications: a systematic review and meta‐analysis. Colorectal Disease. 2014 Jun;16(6):O189-96. Read it!
- Strate LL, Liu YL, Huang ES, Giovannucci EL, Chan AT. Use of aspirin or nonsteroidal anti-inflammatory drugs increases risk for diverticulitis and diverticular bleeding. Gastroenterology. 2011 May 1;140(5):1427-33. Read it!
- Carabotti M, Annibale B, Severi C, Lahner E. Role of fiber in symptomatic uncomplicated diverticular disease: a systematic review. Nutrients. 2017 Feb;9(2):161. Read it!
- Dahl C, Crichton M, Jenkins J, Nucera R, Mahoney S, Marx W, Marshall S. Evidence for dietary fibre modification in the recovery and prevention of reoccurrence of acute, uncomplicated diverticulitis: a systematic literature review. Nutrients. 2018 Feb;10(2):137. Read it!
- Papi C, Ciaco A, Koch M, Capurso L. Efficacy of rifaximin in the treatment of symptomatic diverticular disease of the colon. A multicentre double‐blind placebo‐controlled trial. Alimentary pharmacology & therapeutics. 1995 Feb;9(1):33-9. Read it!
- Scarpignato C, Barbara G, Lanas A, Strate LL. Management of colonic diverticular disease in the third millennium: Highlights from a symposium held during the United European Gastroenterology Week 2017. Therapeutic advances in gastroenterology. 2018 May 18;11:1756284818771305. Read it!
- Ojetti V, Petruzziello C, Cardone S, Saviano L, Migneco A, Santarelli L, Gabrielli M, Zaccaria R, Lopetuso L, Covino M, Candelli M. The use of probiotics in different phases of diverticular disease. Reviews on Recent Clinical Trials. 2018 Jun 1;13(2):89-96. Read it!
- Strate LL, Morris AM. Epidemiology, pathophysiology, and treatment of diverticulitis. Gastroenterology. 2019 Apr 1;156(5):1282-98. Read it!
- Ceresoli M, Bianco GL, Gianotti L, Nespoli L. Inflammation management in acute diverticulitis: current perspectives. Journal of inflammation research. 2018;11:239. Read it!
- Kawada T. Risk Factors of Diverticulitis With Special Reference to Inflammation. Clinical Gastroenterology and Hepatology. 2021 Jan 1;19(1):207-8. Read it!
- Turner GA, O’Grady M, Frizelle FA, Eglinton TW, Sharma PV. Influence of obesity on the risk of recurrent acute diverticulitis. ANZ journal of surgery. 2020 Oct;90(10):2032-5. Read it!
- Liu PH, Cao Y, Keeley BR, Tam I, Wu K, Strate LL, Giovannucci EL, Chan AT. Adherence to a healthy lifestyle is associated with a lower risk of diverticulitis among men. The American journal of gastroenterology. 2017 Dec;112(12):1868. Read it!
- Schieffer KM, Kline BP, Yochum GS, Koltun WA. Pathophysiology of diverticular disease. Expert review of gastroenterology & hepatology. 2018 Jul 3;12(7):683-92. Read it!


