Heartburn, indigestion, and other gastrointestinal issues can be caused by GERD or acid reflux. Learn all about acid reflux and what can be done to prevent or treat it.
When you suffer from acid reflux, the gastrointestinal regions handling stomach acids are not working optimally. As a consequence, you may experience heartburn, acid indigestion, discomfort when swallowing, and other problems.
Below we give a comprehensive overview of GERD or acid reflux and describe how to improve your gastrointestinal health when you are affected by this condition.
What is GERD or acid reflux?
GastroEsophageal Reflux Disease, or GERD is a chronic form of acid reflux, which occurs when a person suffers from acid reflux symptoms at least twice a week. If you have been diagnosed with GERD or chronic acid reflux, partially digested contents from the stomach, containing gastric acids, move up from the stomach and into the oesophagus. The condition is also known as acid regurgitation or gastroesophageal reflux.
How does GERD or chronic acid reflux happen?
GERD or acid reflux occurs when the lower oesophageal sphincter, a valve-like organ at the end of the oesophagus, does not close properly after food reaches the stomach. With this malfunction in place, the content of the stomach, partially digested food and gastric acids, can flow back and up the oesophagus, reaching the throat and even the mouth1.
How common is GERD or chronic acid reflux?
Acid reflux is a common occasional occurrence, affecting everyone at some point of their lives, just like heartburn. However, if your acid reflux and heartburn symptoms occur more than twice per week over several weeks, you may have developed GERD, which is essentially a chronic version of acid reflux and heartburn2. If you think you suffer from GERD, you should visit a health care provider immediately, to have your condition diagnosed and treated. GERD or chronic acid reflux does not normally go away on its own and can lead to more serious health problems.
How many people suffer from GERD or chronic acid reflux?
Worldwide, the prevalence of GERD or chronic acid reflux has been estimated to range between 8% – 33%3. In Australia, one study estimated the prevalence of GP-diagnosed gastro-oesophageal reflux at 11.6%, whereas the general population was estimated to have a slightly lower prevalence of 7.5%4-5. Another study, based on a GP-provided data from 9,156 patients, across multiple chronic conditions in Australia, coincided with a comparable prevalence rate, reporting that about 10% of their patients suffered from GERD or chronic acid reflux6.
Typical symptoms of GERD or chronic acid reflux
Regular heartburn is the most common symptom experienced by someone with GERD or chronic acid reflux, occurring at least twice per week. Also, patients commonly experience acid regurgitation, or a burning feeling in their throat, due to the presence of gastric acids7. Other symptoms, however, may also be present, such as
This is a common symptom, which can be so severe that it might be mistaken by a heart attack. Anyone experiencing chest pain for more than a few minutes should seek immediate medical attention.
also known as dysphagia, this condition affects about one in three people with GERD, particularly when trying to eat solid foods, like meat or bread.
Symptoms include a persistent cough, which may worsen at night, wheezing, tooth decay and gum disease, laryngitis, (inflammation of the larynx), bad breath and bloating.
What are symptoms of GERD or chronic acid reflux in children?
Infants and children can also develop GERD or chronic acid reflux. It is estimated that about two-thirds of 4-month-old babies develop GERD or chronic acid reflux symptoms and up to 10 percent of 1-year-old babies are affected by GERD or chronic acid reflux. A recent study identified three main classes of symptoms that can help clinicians diagnosed GERD or chronic acid reflux in children8. These main classes of symptoms were:
- Airway flow – which includes stertor, stridor, cyanotic spells
- Airway irritation – including frequent cough, recurrent croup, throat clearing
- Feeding - which include dysphagia, failure to thrive, frequent emesis
Other symptoms may include:
- Frequent small vomiting episodes
- Excessive crying, not wanting to eat (in babies and infants)
- Breathing difficulties
- Frequent sour taste of acid, especially when lying down
- Sore throat
- Feeling of choking that may wake the child up
- Bad breath
- Difficulty sleeping after eating, especially in infants
In young children, however, the presence of GERD or chronic acid reflux usually does not require investigation or therapy. Older children exhibiting typical symptoms of GERD or chronic acid reflux may benefit from treatment with proton pump inhibitor9.
Does a child require hospitalisation from GERD or chronic acid reflux?
- Poor weight gain
- Cyanosis (a bluish or purplish discoloration of the skin due to deficient oxygenation of the blood)
- Excessive irritability
- Excessive vomiting/dehydration
Children exhibiting one or more of these symptoms should be seen by a doctor for further evaluation8.
What treatments are available for a child with GERD or chronic acid reflux?
The first approach may involve an evaluation of your child’s medical history, to identify any potential triggers, such as certain foods. If further treatment is required, your child may need to:
- Take certain over-the-counter or prescription medications
- Change certain body positions, like keeping an upright position after eating
- Receive surgery, but only as a last resort, once specific targets have been identified and other approaches have not worked
Chronic heartburn or a heart attack?
Unfortunately, the symptoms can be similar between these two conditions, as both cause chest pain. Heart burn caused by GERD or chronic acid reflux is a burning sensation that starts in the chest and can radiate to the neck and throat. In contrast, a heart attack can cause a more complex set of symptoms, including pain in the arms, neck and jaw, shortness of breath, sweating, nausea, dizziness, extreme fatigue and anxiety.
However, if you suffer from GERD or chronic acid reflux, and have experienced no results from taking your medications, you should contact a health practitioner immediately.
What are the main causes behind GERD or chronic acid reflux
First, it should be noted that GERD or chronic acid reflux is not caused by excess or altered levels of gastric juices. From a physiological standpoint, GERD or chronic acid reflux occurs because of a malfunction of the lower esophageal sphincter (LES), a valve-like structure that separates the lower end of the esophagus from the stomach.
Under normal conditions, the LES opens to allow for the passage of food into the stomach or to allow for the passage of air from the stomach to the mouth, when we burp. In any other circumstances, the LES should remain closed, preventing any stomach acids from reaching the upper sections of the gastrointestinal tract.
A more important question is what causes the LES to malfunction, leading to GERD or chronic acid reflux. The main factors explaining why LES malfunctions are:
Pressure on the stomach causes bloating or gastric distention, which forces stomach contents (food plus acids) through the LES and into the esophagus. This is why, for example, pregnant women often experience heartburn. Studies also point at obesity as a driving factor, with the same mechanism in play10-11.
Under normal circumstances, stomach acids have a very low pH, or 3 or less, which kills most bacteria. But, when there are low levels of gastric acids or the pH is above 3, bacterial overgrowth can occur. It has been shown in animal models that the inability to produce appropriate levels of gastric acids leads to bacterial overgrowth, which is associated with inflammation and the formation of pre-cancerous polyps12.
This is a problem where people produce low levels of gastric acids. Stomach acids are important for the digestion and absorption of carbohydrates. These acids promote the release of pancreatic enzymes into the small intestine. If there is sub-optimal production of stomach acids, leading to an elevated pH, then carbohydrates will not be digested (broken down) properly
What are risk factors of GERD or chronic acid reflux?
Certain conditions have been shown to increase the chances of developing GERD or chronic acid reflux, including:
- Obesity
- Pregnancy
- Hiatal hernia
- Connective Tissue Disorders
Certain lifestyle choices can also increase your risk of GERD or chronic acid reflux, including:
- Smoking
- Eating large meals
- Lying down or going to sleep shortly after eating
- Eating certain types of foods, such as deep fried or spicy foods
- Drinking certain types of beverages, such as soda, coffee, or alcohol
- Using nonsteroidal anti-inflammatory drugs (NSAIDS), such as aspirin or ibuprofen
For more information on risk factors, see this website.
Some foods have also been found to act as trigger for GERD or chronic acid reflux symptoms. These include:
- High-fat foods
- Spicy foods
- Chocolate
- Citrus fruit
- Pineapple
- Tomato
- Onion
- Garlic
- Mint
- Alcohol
- Coffee
- Tea
- Soda
To learn more about foods that can potentially trigger GERD symptoms, see this website.
Other food products that should be avoided include fructose and artificial sweeteners, processed foods, alcohol and water during meals.
Some foods that can help reduce GERD symptoms include:
- Nutrient-dense and whole foods
- Fermented foods with probiotics
- Bone broth
To learn more about foods to eat and foods to avoid if you suffer from GERD or chronic acid reflux, see this website.
Do you have GERD or chronic acid reflux?
If you experience heartburn often, more than twice per week, you should consider consulting with a health care provider. Chronic heartburn and acid reflux will damage the tissue lining of your esophagus, causing significant pain and discomfort.
Without appropriate management, GERD or chronic acid reflux can affect multiple aspects of your life, such as your eating and sleeping habits. For example, GERD or chronic acid reflux can lead to constant pain when eating and difficulty sleeping.
The GERD (chronic acid reflux) – Asthma connection
Studies have shown that about 75% of people with asthma also suffer from GERD or chronic acid reflux and having asthma increases your chances of developing GERD two-fold, compared to the normal population14.
This connection, however, is not clearly understood, but a common theory proposes that changes in pressure at the levels of the thorax of asthmatic patients lead to more acid reaching into the esophagus. Also, certain asthma medications may affect the function of the LES, promoting acid reflux15.
If you or your child suffers from asthma and exhibit GERD symptoms, a visit to a health care provider may help manage both conditions and find a treatment pathway that can help improve symptoms.
Can GERD or chronic acid reflux be fatal?
Studies have shown that about 75% of people with asthma also suffer from GERD or chronic acid reflux and having asthma increases your chances of developing GERD two-fold, compared to the normal population14.
This connection, however, is not clearly understood, but a common theory proposes that changes in pressure at the levels of the thorax of asthmatic patients lead to more acid reaching into the esophagus. Also, certain asthma medications may affect the function of the LES, promoting acid reflux15.
If you or your child suffers from asthma and exhibit GERD symptoms, a visit to a health care provider may help manage both conditions and find a treatment pathway that can help improve symptoms.
On its own, GERD or chronic acid reflux is not a life-threatening condition. However, on the long term, GERD can lead to complications, such as
This occurs when gastric acids cause irritation and inflammation in the lining of the esophagus, potentially causing ulcers in the esophagus, heartburn, chest pain, bleeding and trouble swallowing
This occurs when there is long-term damage to the cells of the eosophagus. This condition is a risk factor for cancer of the esophagus.
There are two main types.
- Adenocarcinoma, which usually develops in the lower part of the esophagus. Barrett’s esophagus can be the starting point.
- Squamous cell carcinoma, which begins in the cells that line the esophagus, affecting the upper and middle part of the esophagus.
This happens when parts of the esophagus develop scars from the damage sustained by acid reflux. These scars represent non-functional tissue and can affect normal eating and drinking3.
How is GERD and chronic acid reflux diagnosed?
Evaluation of your medical history is the usual first step to establish the presence and frequency of acid reflux. To reach a final diagnosis of GERD or chronic acid reflux, a clinician will rely in one or more of the following tests:
- X-ray tracking – after drinking a barium solution, X-ray imaging can help your doctor examine your upper digestive tract;
- upper endoscopy – here a flexible tube fitted with a camera is inserted into your esophagus to examine it and collect a small piece of tissue, if required;
- esophageal manometry – in this approach a tube is threaded into the esophagus. The goal is to measure the strength of the esophageal muscles;
- esophageal pH monitoring – here, a monitoring device is inserted into the esophagus, which will inform when stomach acid enters.
What medications are recommended for GERD or chronic acid reflux?
Making certain lifestyle changes can help reduce or relieve GERD symptoms. There are also certain medications for GERD or chronic acid reflux that can be used, some of which are available over-the-counter. Some common examples include:
- antacids;
- H2 receptor blockers;
- proton pump inhibitors (PPIs).
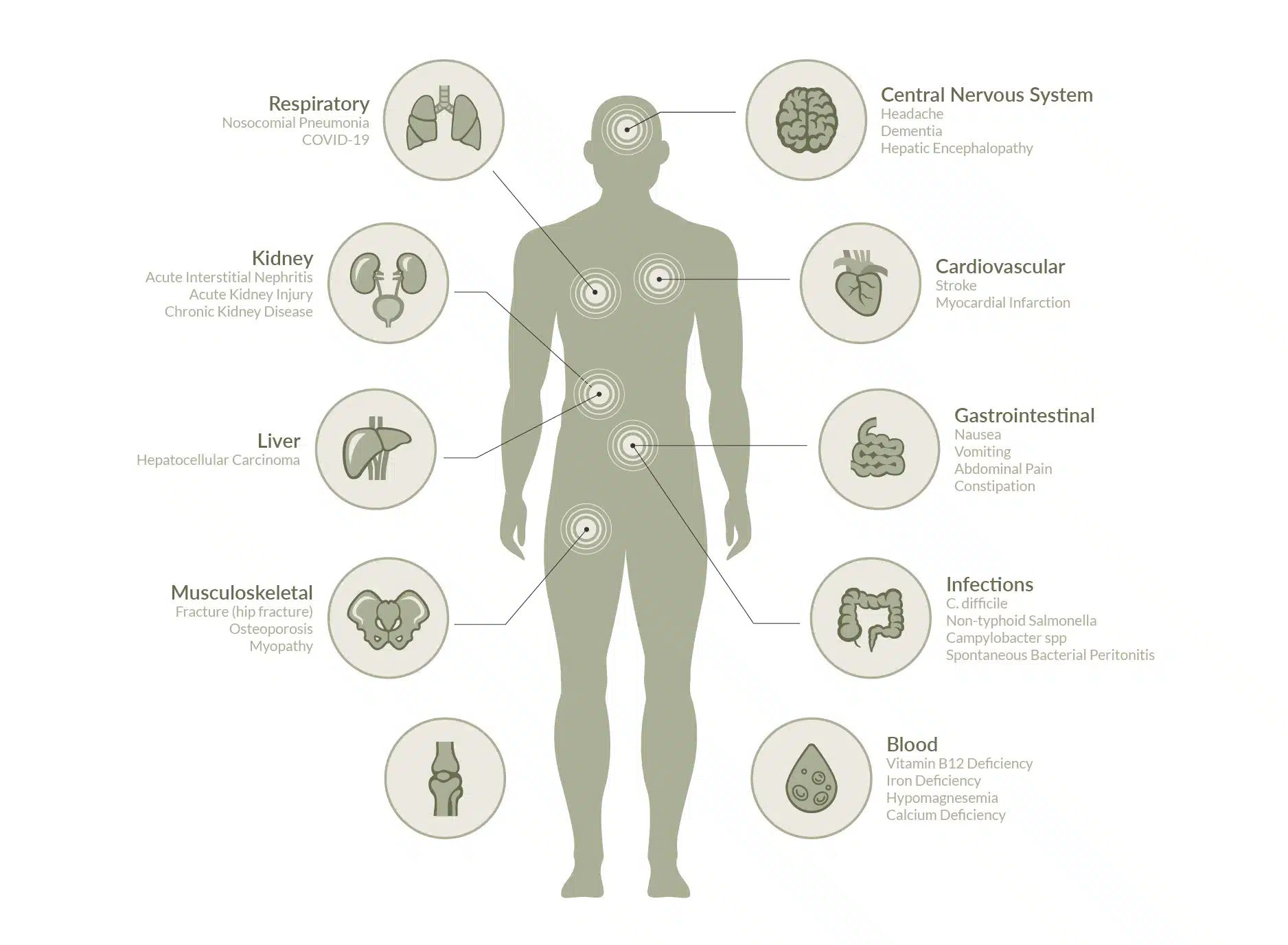
However, caution should be taken when using these medications16-18. PPIs, for example, are associated with multiple health problems, including:
- Alteration of the Gut Microbiota;
- Impairment of Nutrient Absorption;
- Increasing the Risk of Cardiovascular Events;
- Potentially damaging the Kidneys;
- Negatively Affecting Cognitive Function.
For more information about risks of over-the-counter medications for GERD, see this website, and this one too.
Is surgery for GERD or chronic acid reflux a good option?
In most cases GERD can be managed with medications and lifestyle changes. Surgery is a last resort option, and can involve:
- Fundoplication – this is a common surgical treatment for GERD that tightens and reinforces the LES;
- TIF (Transoral Incisionless Fundoplication) – This procedure creates a barrier between the stomach and the esophagus, which prevents reflux of stomach acid;
- LINX device implantation -The LINX device is a ring of tiny magnets that can keep the junction between the stomach and esophagus closed to prevent acid reflux, while allowing food to enter the stomach.
For more information about potential surgical procedures for GERD, see this website.
Can I prevent GERD or chronic acid reflux?
The best approach to prevent GERD is to make significant changes to your lifestyle. This may include:
- Having a healthy weight;
- Eating small, frequent meals;
- Reducing fat consumption;
- Sitting upright while eating and staying upright for 45 to 60 minutes afterward;
- Avoid eating before bedtime;
- Try not to wear clothes that are tight in the abdomen;
- Stop smoking;
- Eliminate possible trigger foods.
Another important approach involves changes in lifestyle that target three specific goals:
- Reduce factors that promote bacterial overgrowth in the stomach and decrease stomach acid;
- Improve stomach acid, enzymes and nutrients, as these are key for optimal digestion;
- Restore beneficial gut bacteria.
Modern Functional Medicine and GERD (chronic acid reflux)
At AUSCFM, our team of doctors and health practitioners use an evidence-based, comprehensive approach for the treatment of GERD or chronic acid reflux and all associated symptoms. Our approach is based on extensive testing, including laboratory tests of blood, breath, stool and urine. We also rely on extensive patient consultation, as well as investigation aimed at identifying the specific drivers of your condition.
Our main goal is to identify and treat the underlying causes behind GERD or chronic acid reflux.
understand what is driving your GERD or acid reflux and find an effective solution
References
- Dickman R, Fass R. The pathophysiology of GERD. InGastroesophageal Reflux Disease 2006 (pp. 13-22). Springer, Vienna. Read it!
- Delshad SD, Almario CV, Chey WD, Spiegel BM. Prevalence of gastroesophageal reflux disease and proton pump inhibitor-refractory symptoms. Gastroenterology. 2020 Apr 1;158(5):1250-61. Read it!
- Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout AJ, Vaezi M, Sifrim D, Fox MR, Vela MF, Tutuian R. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018 Jul 1;67(7):1351-62. Read it!
- Miller G, Wong C, Pollack A. Gastro-oesophageal reflux disease (GORD) in Australian general practice patients. Australian family physician. 2015 Oct;44(10):701. Read it!
- Harrison C, Britt H, Miller G, Henderson J. Prevalence of chronic conditions in Australia. PLoS ONE 2013;8:e67494. Read it!
- Knox SA, Harrison CM, Britt HC, Henderson JV. Estimating prevalence of common chronic morbidities in Australia. Medical Journal of Australia. 2008 Jul;189(2):66-70. Read it!
- Cohen E, Bolus R, Khanna D, Hays RD, Chang L, Melmed GY, Khanna P, Spiegel B. GERD symptoms in the general population: prevalence and severity versus care-seeking patients. Digestive diseases and sciences. 2014 Oct 1;59(10):2488-96. Read it!
- Carr MM, Nguyen A, Nagy M, Poje C, Pizzuto M, Brodsky L. Clinical presentation as a guide to the identification of GERD in children. International journal of pediatric otorhinolaryngology. 2000 Aug 11;54(1):27-32. Read it!
- Poddar U. Gastroesophageal reflux disease (GERD) in children. Paediatrics and international child health. 2019 Jan 2;39(1):7-12. Read it!
- Locke GR 3rd, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ 3rd. Risk factors associated with symptoms of gastroesophageal reflux. Am J Med. 1999 Jun;106(6):642-9. Read it!
- Sugerman HJ. Increased intra-abdominal pressure and GERD/Barrett’s esophagus. Gastroenterology. 2007 Dec 1;133(6):2075. Read it!
- Friis-Hansen L, Rieneck K, Nilsson HO, Wadström T, Rehfeld JF. Gastric inflammation, metaplasia, and tumor development in gastrin-deficient mice. Gastroenterology. 2006. Read it!
- Austin GL, Thiny MT, Westman EC, Yancy WS Jr, Shaheen NJ. A very low-carbohydrate diet improves gastroesophageal reflux and its symptoms. Dig Dis Sci. 2006 Aug;51(8):1307-12 Read it!
- Parsons JP, Mastronarde JG. Gastroesophageal reflux disease and asthma. Current opinion in pulmonary medicine. 2010 Jan 1;16(1):60-3. Read it!
- Mastronarde JG. Is there a relationship between GERD and asthma?. Gastroenterology & hepatology. 2012 Jun;8(6):401. Read it!
- Jackson MA, Goodrich JK, Maxan ME, Freedberg DE, Abrams JA, Poole AC, Sutter JL, Welter D, Ley RE, Bell JT, Spector TD. Proton pump inhibitors alter the composition of the gut microbiota. Gut. 2016 May 1;65(5):749-56. Read it!
- Heidelbaugh JJ. Proton pump inhibitors and risk of vitamin and mineral deficiency: evidence and clinical implications. Ther Adv Drug Saf. 2013 Jun;4(3):125-33. Read it!
- Yibirin M, De Oliveira D, Valera R, Plitt AE, Lutgen S. Adverse effects associated with proton pump inhibitor use. Cureus. 2021 Jan;13(1). Read it!


